
Past events at MIOT
1st Time in India, MIOT Saves Liver Transplant Patient from Lifelong Dependence on a Biliary Drainage Catheter

Standing from Left to Right:
Dr. Karthikeyan Damodaran, Director, Vascular & Interventional Radiology, MIOT International;
Mrs. Mallika Mohandas, Chairman, MIOT International;
Patient Ms. GULNURA TAABALDYEVNA ZHOROEVA from Kyrgyzstan;
Dr. Karthik Mathivanan, Program Director – Department of Liver & Multi-Organ Transplant & HPB Surgeon, MIOT International;
Dr. Palaniappan S, Senior Medical Gastroenterologist, Hepatologist & Interventional Endoscopist, MIOT International.
MIOT International treats a post-liver-transplant patient with bile duct blockage using two tiny magnets, restoring bile flow and avoiding high-risk reconstructive surgery.
MIOT gave a 43-year-old mother of two from Kyrgyzstan a second lease at life with a liver transplant, but that happiness didn’t last for long.
During a living donor liver transplant, the surgeons usually take a portion of the donor’s liver along with its blood vessels and bile duct. These are then carefully stitched and connected to the recipient’s body so the new liver can function normally. For most patients, this healing process is uneventful, and these delicate connections recover without any complications.
But not every threat announces itself. The tiny passage that carries bile from the liver to the intestine, called the bile duct, heals naturally after it is surgically connected during a liver transplant. As this healing takes place internally, scar tissue can sometimes build up around the connection, gradually narrowing or completely blocking the bile duct. This narrowing can put everything at stake – a small structure with the power to cause life-threatening complications. It is one of the most common complications after a liver transplant, affecting 40% of the patients.
Fifteen months later, that complication became a reality for Ms. GulnuraTaabaldyevnaZhoroeva. She came to MIOT with severe itching and jaundice. On evaluation, a complete blockage of the bile duct was found, preventing the normal flow of bile from the liver. If left untreated, it could cause severe bile duct infection, life-threatening sepsis, and eventual failure of the transplanted liver.
While most patients can be treated using standard minimally invasive procedures, Ms. Gulnura’s case was different. Her bile duct had completely sealed shut. Despite multiple attempts, doctors were unable to cross the blockage or place a stent.
When every conventional treatment failed
The multidisciplinary team at MIOT first attempted every established treatment.
Doctors first attempted an Endoscopic Retrograde Cholangiopancreatography (ERCP), a minimally invasive procedure performed through the mouth to reach and open the blocked bile duct.
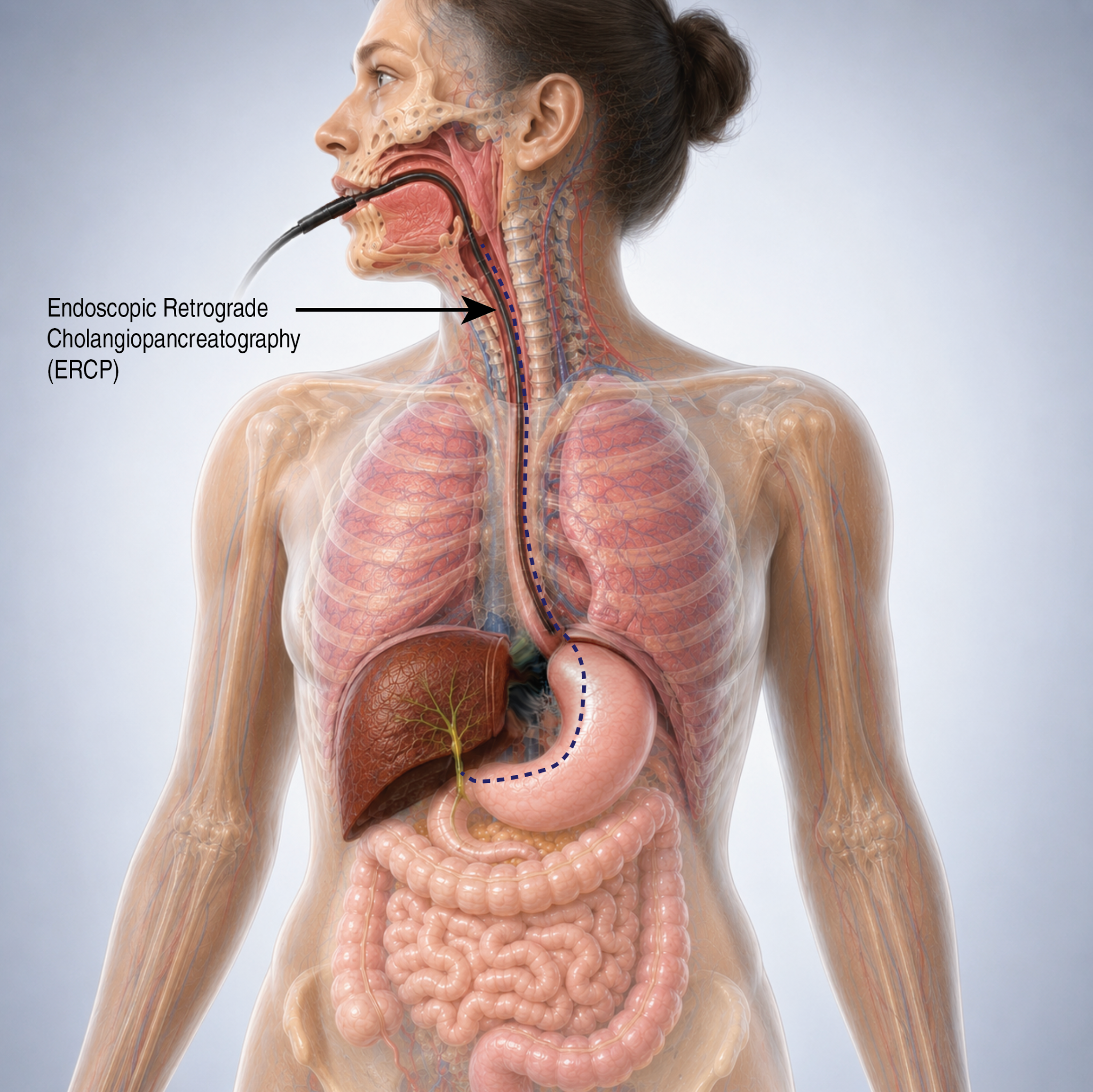
Endoscopic Retrograde Cholangiopancreatography (ERCP)
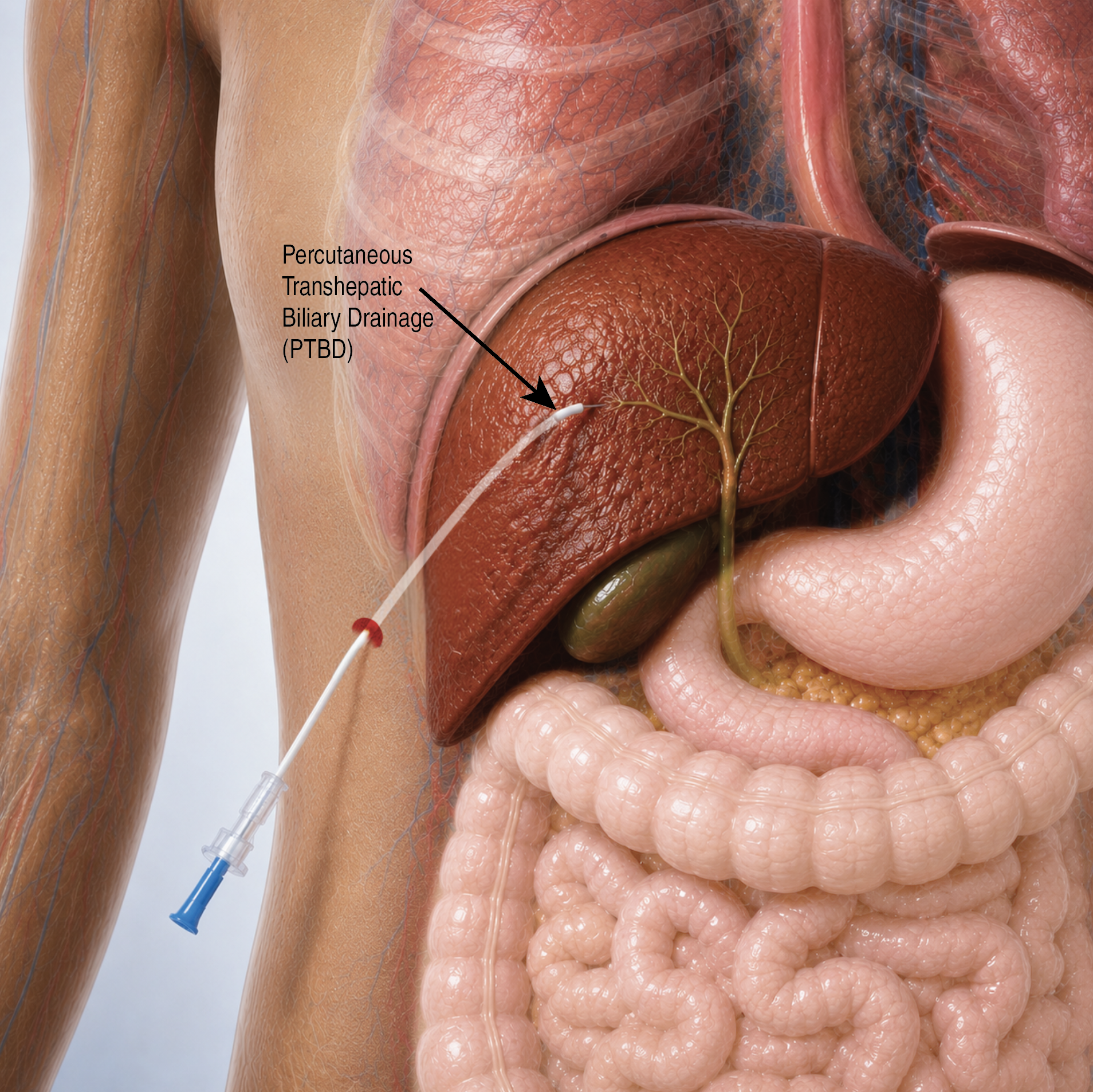
Percutaneous Transhepatic Biliary Drainage (PTBD)
They also carried out a Percutaneous Transhepatic Biliary Drainage (PTBD), an image-guided procedure in which a thin tube is inserted through the skin and liver into the bile duct. Despite repeated attempts, neither approach could cross the blockage because the bile duct had completely sealed shut, leaving no passage to reopen.
To protect the transplanted liver, the team inserted an external biliary drainage catheter. This allowed bile to drain outside the body while preventing further liver damage.
Quality of Life Concerns with Prolonged Drainage Tube
Although effective, the tube had a significant impact on her daily life. Without another solution, she could have remained dependent on long-term external bile drainage or required a major reconstructive surgery.
Why Reconstructive Surgery After Transplant Is High-Risk
Revision surgery after a liver transplant is among the most challenging procedures. Dense scar tissue around the transplanted liver makes the operation technically demanding. It also carries a higher risk of complications, prolonged recovery and, in difficult cases, even loss of the transplanted organ.
An innovative solution using two tiny magnets
Determined to find a safer alternative, the multidisciplinary team, including the liver transplant team, interventional radiologists, therapeutic endoscopists, anaesthesiologists, and other medical professionals, together planned an innovative technique called Magnetic Compression Anastomosis (MCA), a procedure that uses two tiny magnets.
This exceptionally rare and innovative procedure has been performed only at a handful of elite medical institutions worldwide, predominantly in South Korea and Japan. With this case, MIOT becomes the 1st in India to treat a completely blocked bile duct following a liver transplant using this innovative technique.
Rewriting Treatment with Two Tiny Magnets
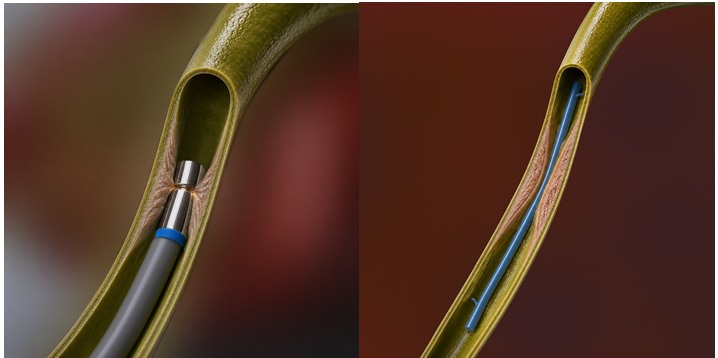
In this procedure, a gastroenterologist placed a magnet through an endoscope from inside the intestine. At the same time, the second magnet was guided through the existing drainage tract from outside the body by an interventional radiologist. The magnets are carefully positioned on either side of the blocked bile duct.
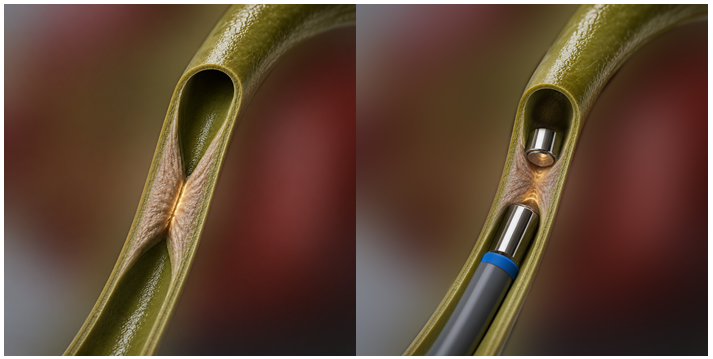
Over time, the magnets gently attract each other. Their constant magnetic force compresses the scar tissue between them. This gradually creates a new channel through the blocked segment, allowing bile to flow naturally once again.
The entire procedure avoids reopening the abdomen and eliminates the need for major reconstructive surgery.
A second chance at normal life
The procedure was successful. Normal bile flow was restored. The external drainage catheter was removed.
Today, Ms. Gulnura is symptom-free. Her transplanted liver is functioning well. Most importantly, she no longer depends on an external drainage tube and has returned to her normal daily life.
A milestone in liver transplant care
This landmark case demonstrates MIOT’s expertise in managing some of the most complex complications after liver transplantation. It also highlights the strength of close collaboration between liver transplant surgeons, interventional radiologists and therapeutic endoscopy specialists.
By successfully using Magnetic Compression Anastomosis after all conventional treatments had failed, MIOT has opened a new possibility for treating complex bile duct Strictures in patients. This achievement marks an important milestone in liver transplant care in India. It reinforces MIOT’s commitment to bringing globally advanced, minimally invasive innovations to patients when they need them the most.
Who Can Benefit From Magnetic Compression Anastomosis (MCA)
- Patients with complete bile duct blockage: Where the bile duct is fully sealed, and conventional procedures cannot restore flow.
- Living Donor Liver Transplant (LDLT) recipients: Patients who develop bile duct narrowing or blockage after transplant surgery.
- Patients for whom repeat surgery is high-risk: Especially when scar tissue or complex anatomy makes revision surgery unsafe or difficult.
- Patients dependent on external biliary drainage: Patients with persistent jaundice, poor quality of life, and dependence on a biliary drainage catheter.