

Treatments & Procedures
Permanent Pace-maker Implantations (PPI)
Permanent Pacemaker Implantation (PPI) may be in the form of Single Chamber (VVI; VVIR) pace maker implantation, Dual Chamber (DDD; DDDR) pace-maker implantation and Cardiac re-synchronization therapy (CRT).
Why does one need a Permanent pace-maker?
Every heart has an in-built battery called the Sino-atrial node or SA node and a wiring system of its own, which generates electrical impulses which when conducted to the heart muscle, makes it to beat or contract and thereby ensuring that the brain and the different parts of the body get enough blood to function normally. The normal range of the number of beats generated by the SA node is 60 to 100 per minute. When there is a gross failure of the SA node and rates are much less than 50 per minute (Bradycardia), the heart fails to generate sufficient blood supply to the brain which can result in giddiness and or loss of consciousness/ syncope. Failure of the wiring system also can produce the same effect from heart blocks called AV blocks or complete heart blocks. When such conditions arise, it becomes imperative that the appropriate number of heart beats is generated with the use of implanted batteries or pulse-generators with wires introduced into the heart by a procedure called Permanent pace-maker implantation.
What is Permanent Pace-maker Implantation and how is it performed?
Permanent pace-maker implantation involves placement of a single wire or lead (Single Chamber PPI) into the Right ventricular chamber of the heart (VVI; VVIR) or two wires or leads (Dual Chamber PPI), one each into the Right ventricle and the Right atrial chamber of the heart (DDD; DDDR). The entire procedure is done under local anaesthesia and the patient is conscious during the procedure. The lead or leads are introduced into the heart usually via a small needle puncture or punctures into the left axillary vein or subclavian vein, below the collar bone or clavicle. The lead or leads are then connected to a battery or pulse-generator, which is thereafter placed inside a small surgical pocket created under skin and tissue below the collar bone. This pocket is the closed with sutures or stitches, in layers. The patient is then discharged usually on the third day following the procedure. Periodic follow up and programming is required and the battery usually lasts from 8 to 12 years depending on the dependency of the patient on the pace-maker.
The procedure is however not free of complications. There is a risk of pneumothorax, bleeding and infection from the procedure, which are generally much less in the hands of the experienced.
CRT also uses leads and pulse generators as above, but the indications for CRT are totally different and would be discussed separately.
Single Chamber Pace-maker
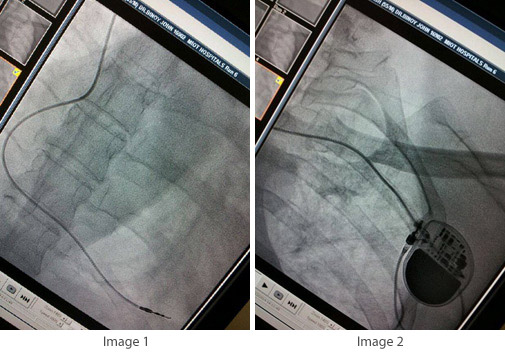
Image 1: Shows a single lead placed (screw-in lead) in the Right Ventricle of the Heart.
Image 2: Shows the battery or the Pulse-generator placed under the skin and tissue via a surgical pocket. The single RV lead is shown connected to the PG.
Dual Chamber Pace-maker
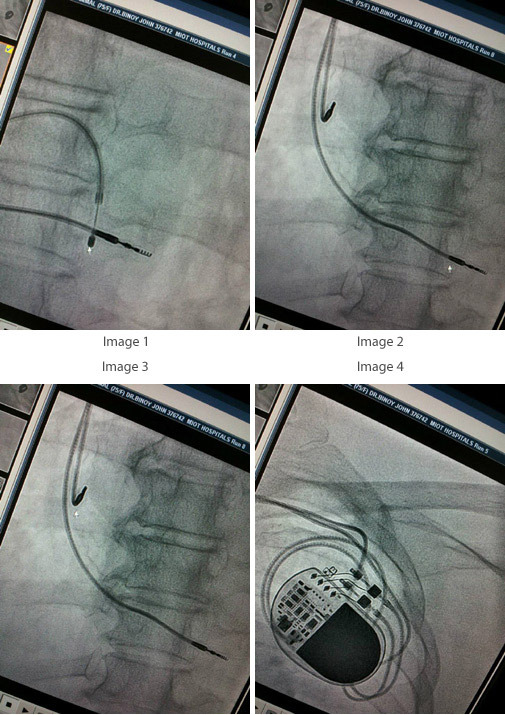
Image 1: Arrow shows a temporary pace-maker lead placed inside the Right ventricular chamber of the heart, which acts a s a back-up till the permanent pace-maker is implanted.
Image2: Arrow shows the permanent lead screwed inside the Right ventricular chamber of the heart.
Image3: Arrow shows the permanent lead screwed inside the Right atrial chamber of the heart.
Image4: Arrow shows the battery or the pulse-generator into which both the leads are connected. The battery is placed under the skin and tissue via a surgical pocket.